
Introduction
WHO defines health as “ A state of complete physical, mental and social well being and not merely absence of disease or infirmity. It is not an absolute state, but a relative concept. Clinicians depend on the laboratory test results for diagnosis, prognosis and ruling out diseases in addition to clinical examination. The medical laboratory data is interpreted with the help of reference values for all the tests performed in the clinical chemistry laboratories. Reference intervals are typically defined as intervals where 95% of test results of healthy individuals occur.1 According to IFCC it is necessary for every lab to have their own set of reference limits. Establishing reference intervals is a difficult and expensive affair and for the same reason most of the clinical laboratories adopt to reference values provided by Kit manufacturers, journals, text books, western cohorts.2 It provides no information on the reference population and even if it does, would most likely be of the Caucasian population.
These reference intervals can be questioned because the biochemical parameters are influenced by ethnicity, ecological factors like climate, altitude, life style dietary habits as well as physical activity. India is a country with extreme variations compared to western countries. The laboratory should establish population-based reference intervals for appropriate analysis of test reports.3
Kidney function is evaluated using a variety of tests and procedures which help to determine whether it is functioning properly. The study done by international society of nephrologists, kidney disease data center reported a recent increase in prevalence of kidney disease from 13% to 17%.4
The lifestyle, ethnicity, dietary factors, epigenetic mechanisms influence the body size and weight which corresponds to renal volume and hence renal function.5 So there is a need to validate reference intervals in our population.
To our knowledge there is not much population based studies on reference intervals of renal profile parameters in India. The aim of this study is to establish reference values for some renal function test parameters and to determine possible difference between published and local reference ranges.
Materials and Methods
This study was undertaken at Ambalappuzha North Grama panchayath which is a coastal area in the Alappuzha district of Kerala. Apparently healthy individuals of both sex aged between 18-60 years who attended a health camp organised by Department of Biochemistry, Govt TD Medical college in association with the Ambalappuzha north grama panchayath in the month of February 2018 were included in the study. Study was conducted as per ICMR guidelines and also by the specific instructions given by IEC.EC27/2017 dated 23/3/2017. The healthy volunteers from different wards of the Grama Panchayath were included in the study based on CLSI/NCCLS6 guidelines. The following individuals were excluded
·Individuals with pathophysiological states like renal failure, congestive heart disease, chronic respiratory disease, liver disease, malabsorption syndromes, nutritional anemia, infections Systemic diseases-Hypertension, Diabetes Mellitus, Hyperthyroidism. Intake of pharmacologically active agents-Alcohol, tobacco, OCP, replacement or supplementation therapy- eg. insulin, nephrotoxic drugs like chronic NSAIDS usage, Aminoglycoside antibiotics, Anticancer drugs, Antipsychotics, steroids and other hyperglycemic agents.
Modified physiological states - pregnancy, psychological and mental disorders such as severe stress and depression, exercise or physical training, food intake prior to blood collection
Other factors - obesity (Body Mass Index >30 kg/m2)
Samples were collected between 8 am and 9.30 am after overnight fasting for 10-12 hours. Under aseptic precautions 2 ml sample was collected in plain tubes with gel. Cold chain was maintained throughout sample collection and analysis and the samples were analysed on the same day. Analysis was done in fully automated analyser Beckmann Coulter Au 486 with closed system pack reagents. All icteric, hemolytic and lipemic samples were identified and were not processed. The study variables measured were serum urea by urease, serum uric acid by uricase and serum creatinine by modified Jaffes method. Methods used were all IFCC recommended. The study incorporated internal QC materials (biorad bi-level) and EQAS from CMC Vellore .The Coefficient of Variation and Z score for the parameters noted were within the acceptable limits.
Statistical analysis
The non parametric methodology for determination of Reference interval is adopted in the study as recommended by IFCC and NCCLS.7 Median, central 95 percentile and 90 % confidence interval were calculated. The 97.5 percentile and 2.5 percentile formed the upper and lower reference limits of the population. Statistical analysis was done using SPSS Version 16. The higher value outliers were excluded using Q3+ 1.5 Interquartile range and the lower value outliers were excluded using Q1-1.5 Interquartile range. The selected reference individuals may be further sub classified into more homogenous groups by stratifying them according to age and sex.
Table 1
Reference interval for Urea among the study population
Table 2
Reference interval for Uric acid among the study population
Table 3
Reference interval for Creatinine among the study population
Results and Discussion
A total of 441 apparently healthy adults who enrolled for a free medical camp conducted by department of biochemistry, Govt. TD Medical college, Alappuzha in association with Amabalappuzha North Grama Panchayath were included in the study. Out of the 44 1, 266 were females (60.22%) and 175 were males (39.78%) aged between 18 to 60 yrs.
The results for the selected parameters (Urea, Uric acid, Creatinine) of target population are tabulated in the Table 3, Table 2, Table 1 respectively.
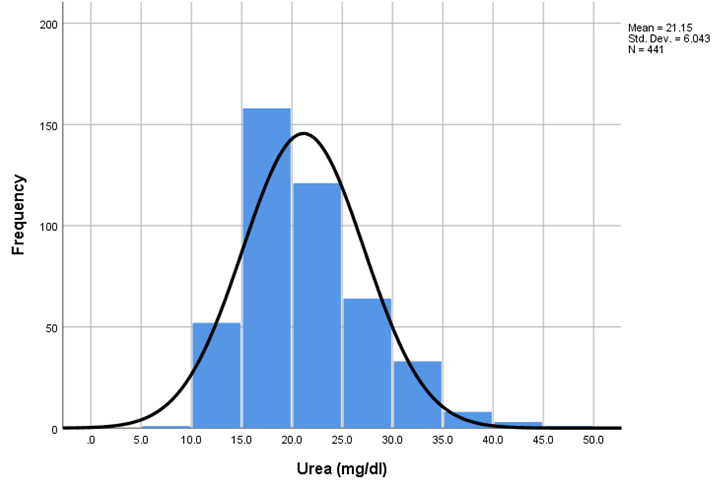
The Frequency histograms of Urea, Uric acid and creatinine values of target population are depicted in the figure 1 ,2,3 respectively.
The serum urea values are 21.15 +/- 6.04 mg/dl with 2.5th percentile 12.51 and 97.5th percentile 35.38. The mean, SD and reference interval for Uric acid (in mg/dl) is 4.86,1.41,2.38-7.39 in males and 4.28,0.95,2.69-6.7 in females and for creatinine (in mg/dl) is 0.93,0.15,0.67-1.27 in males and 0.80 ,0.12 ,0.61-1.10 in females respectively .The standard reference intervals from the pack insert used in our lab are urea 17-43 mg/dl, Uric acid 3.5-7.2 mg/dl in males and 2.6-6 mg/dl in females, creatinine 0.84-1.25 mg/dl in males and 0.66-1.09 mg/dl in females respectively.
The Reference range established in the present study were on par with the pack inserts in case of uric acid and creatinine with minimal differences, but Reference intervals for urea showed much difference from conventional pack inserts. It is observed that Reference Interval for urea is lower than standard Reference interval, both Lower limit and upper limit. The Reference interval for Uric acid is much wider than established Reference interval with lower cut off for lower limit and higher cut off for upper limit in males where as in case of females, both limits were slightly higher than standard Reference interval. No much wider difference was noted for creatinine, but the lower Reference limit was slightly lower than standard Reference limit in both males and females.
It is observed that there is a gradual increase of mean of urea and creatinine as the age advances. The uric acid mean is high in 30-45 years compared to other two groups in males but a gradual increase in mean was noted in females on advancing age.
In the study conducted by Tester F Ashavaid and co workers at Hinduja National hospital and Medical research Mumbai to establish Reference intervals, the Urea, Uric acid and creatinine values were 10.7-36.4mg/dl,10.7-34.2 mg/dl; 3.8-7.8 mg/dl, 2.6-6.3 mg/dl ;0.7-1.3 mg/dl,0.6-1 mg/dl in males and females respectively which coincided with our study.8 According to the study conducted by Mascha Verma and co-workers at SRL Ranbaxy laboratory Mumbai, the reference interval of creatinine was 0.7-1.3 mg/dl in males and 0.4-1 mg/dl in females which showed the lower limit slightly on lower side than established limit.9 Sundaram M. and others conducted a study of 213 subjects on healthy individuals attending a HIV referral centre in Chennai. According to this study, reference interval for Serum urea, serum uric acid, Serum creatinine in males were 9-33 mg/dl,3.1-8.3 mg/dl, 0.9 to 1.3 mg/dl and in females were 9-27 mg/dl,2-5.2 mg/dl, 0.7 to 1.0 mg/dl. The Reference interval of urea and creatinine was at par with our study but uric acid Reference interval was slighty higher in males and lower in females than our study as well as established Reference intervals.10
In another study to establish Reference ranges for serum uric acid among healthy Assamese people conducted by Madhumitha Das and co workers, the observed Reference interval was 3.5-8.7 mg/dl in males and 2.5-6.9 mg/dl in females. Here also Uric acid Reference Intervals were slightly higher than established Reference intervals.11 A progressive increase in Reference ranges of Urea, Uric acid and Creatinine with advancing age was noted in the study conducted by Dharmaveer Yadav and co workers in the North Indian population.12 In the study conducted by Aono T and co workers significant positive correlation was found between urea levels and age.13
Age and ethnicity related variations in the renal profile parameters were noted among the African population in the study conducted by Shaza.M.Ahamed and co workers and among US population by Jones C.A and co workers.15, 14
Genetic diversity, epigenetic and prenatal factors may have impact on renal volume, number of glomeruli and renal function. Certain studies postulated that the healthy adult Indian population have lower GFR and kidney volume in comparison with other ethnic groups.16 This may be the reason for lower Reference range of urea in the study. The serum uric acid reference range established in this study were higher than the ranges provided by most of the kit insert owing to the strong prominence of the non vegetarian diet on this parameter.17


Conclusion
With this pilot study we can conclude that there exist differences in reference interval for various populations and hence there is a need for larger population studies in the future so that we can extrapolate the same to a larger reference population, and the need for adopting pack insert values can be eliminated for better healthcare.
Author’s contribution
Designed the study: Dr. Rajesh & Dr. Jyothsna S.
Acquisition of Data: Dr. Rajesh and Dr. Jyothsna S.
Managed and Analysed the data : Dr. Rajesh.
Interpreted the data, Drafted and reviewed the article: Dr. Rajesh and Dr. Jyothsna S.
Acknowledgements
Many thanks to the Ambalappuzha North Grama Panchayath authorities and residents who agreed to organize and participate in this study. We are grateful to the staff of Department of Biochemistry, Govt. TD Medical College, Alappuzha for the technical assistance in completion of this project. This study was financially supported by SBMR (State Board of Medical Research).