
Introduction
Diseases of the thyroid gland are common across the world. Thyroid disorders affect 200 million people worldwide, with up to 50% of those with thyroid dysfunction, remaining undiagnosed.1 According to various studies it has been estimated that around 42 million people in India suffer from thyroid disorders like Goiter, Hypothyroidism, Hyperthyroidism, Hashimoto’s disease and carcinoma of the thyroid gland. 2 The global burden of hypothyroidism is significant among the disorders of thyroid gland. In the developed world, hypothyroidism prevalence is approximately 4-5% and that of subclinical hypothyroidism is approximately 4-15%. 3 Thyroid hormones (TH) are necessary for growth and development of the kidney and for the maintenance of water and electrolyte homeostasis.4 The most important function of the thyroid gland is to maintain the homeostasis of the metabolism in the body. 5 Thyroid hormone abnormalities cause marked changes in glomerular and tubular functions and electrolyte homeostasis. Thyroid dysfunction is accompanied by derangement in glomerular filtration; serum creatinine and alteration in the ability of water excretion. 5 The interplay between thyroid and the kidney in each other's functions is known for many years. Thyroid hormones affect renal function by both prerenal and direct renal effects. Pre-renal effects are mediated by the influence of thyroid hormones on the cardiovascular system and the renal blood flow (RBF). The direct renal effects are mediated by the effect of thyroid hormones on glomerular filtration rate (GFR). 6 There is a direct association between hypothyroidism and the impairment of biochemical markers of kidney function compared to euthyroid people. 7 Increasing levels of urea, uric acid, and creatinine and decreasing level of GFR in hypothyroidismpatients. 7 Under normal conditions, daily albumin excretion is in the range of 5–10 mg and the urine albumin: creatinine ratio is in the range of 0–29 mg albumin/g creatinine. Microalbuminuria defined as urine albumin to creatinine ratio of 30 to 299 mg/g (per gram of creatinine) is a valuable marker that predicts endothelial dysfunction. 8 Microalbuminuria is itself associated with endothelial dysfunction and increased risk for cardiovascular morbidity and mortality in high-riskpopulations. 8 Expressing albumin as a ratio to creatinine is desirable as it allows one to use a routine (“spot”) urine sample to detect an abnormal amount of albumin in the urine obviating a 24-hour urine collection. 8 Hence to understand the effect of thyroid disorders on renal function, we estimated and compared serum creatinine, serum urea, urinary creatinine and urinary microalbumin levels with T3, T4 and TSH in hypothyroid patients and euthyroid subjects.
Materials and Methods
This is a Cross-sectional analytical study carried out at Clinical Chemistry Laboratory, at Sir Sayajirao General Hospital (S.S.G.H) and Medical College Baroda, Vadodara. Study subjects were divided into three groups depending upon the levels of the TSH and free T4.
Group-I Euthyroid subjects (n=110)
Group-II Sub clinical hypothyroidism (n=60)
Group-III Overt hypothyroidism (n=50)
Exclusion criteria
Pregnancy
Hypertension
Previously diagnosed cardiovascular
Disorder diabetes mellitus
Acute or chronic infection and inflammation
Previously diagnosed renal diseases like nephrotic or nephritic
Syndrome, nephropathy, urinary tract infection, renal stones, etc. Chronic diseases like tuberculosis, leprosy, acquired
Immunodeficiency syndrome, any autoimmune disorders like rheumatoid arthritis, systemic
Lupus erythematosus, etc.
To select 110 samples for the study, individuals aged 20-70 years were screened during the six-month study period. Subjects with primary hypothyroidism visited the Medicine department at S.S.G Hospital, Vadodara, and their blood and urine samples were collected.
For each patient, fasting blood samples were collected in plain vacutainer (5 ml) and fluoride vacutainer (2ml). The serum was divided into two aliquots: one for thyroid function tests and the other for routine biochemical and renal function tests. A spot urine sample was collected in a clean 100 ml urine collection container and used for urinary albumin and creatinine test.
The chemiluminescent immunoassay (CLIA) was used to measure
TSH level (reference range: 0.35–4.94 mIU/L), fT3level (reference range: 1.53–3.91pg/mL) and fT4 level (reference range: 0.7–1.48 ng/dL) were measured by micro particle enzyme immunoassays.
The fully automatic Erba XL 640 was used to measure
Serum Creatinine was measured by alkaline picrate method. (Reference range: 0.7-1.4 in male & 0.6-1.2 mg/dL in females). Serum Urea was estimated by GLDH (glutamate dehydrogenase) method. (Reference range: 13-45mg/dl). Serum Uric acid measured by Uricase enzymatic Method. (Reference range: 3-7mg/dl). The semiautomatic Micro lab RX-50V was used to measure-Urinary Microalbumin
Estimated GFR (eGFR) using Modification of Diet in Renal Disease (MDRD) formula9
eGFR (ml/min/1.73m2) =175 x ( Standardised serum Creatinine in mg/dl) -1.154x (age in yrs) -0.203
(0.742 if female) (1.210 if African American)
Results
Table 1
Sex distribution in the hypothyroid patients & euthyroid subjects
|
|
Male |
Female |
Total |
|
Sub-clinical Hypothyroid |
14 |
46 |
60 |
|
Overt Hypothyroid |
13 |
37 |
50 |
|
Euthyroid |
27 |
83 |
110 |
Table 2
Age group distribution in the euthyroidsubjects & hypothyroid patients groups
|
Age Group |
Age in Years |
Euthyroid |
Hypothyroid |
|
1 |
20-30 |
42 |
25 |
|
2 |
31-40 |
24 |
31 |
|
3 |
41-50 |
28 |
25 |
|
4 |
51-60 |
10 |
21 |
|
5 |
61-70 |
6 |
8 |
|
Total |
|
110 |
110 |
Table 3
Comparison of mean results for various parameters in three groups: I-Euthyroid, II-Subclinical, and III-Overt Hypothyroid
Table 3 These results wereseen in Free T3, free T4, Serum TSH, urine microalbumin & urinary creatinine, serum creatinine, & serum uric acid were tested on 220 urine & serum samples. Statistical analysis was done on 220samples.
Thyroid Hormones
Mean results of Serum free T3, Serum free T4 & Serum TSH were seen in the Euthyroid subjects, Subclinical & Overt hypothyroid patients.
Serum free T3 2.61±0.48 pg/mL, 2.71±0.86 pg/mL, and 2.17±0.91 pg/mL
Serum free T4: Mean levels were 1.19±0.5 ng/dL, 0.99±0.27 ng/dL and 0.59±0.1 ng/dL.
Serum TSH: Mean levels were 2.46±1.18 mIU/L (Euthyroid), 6.93±1.18 mIU/L and 27.92±23.92 mIU/L.
Statistically significant differences were found in serum levels of T3, T4, and TSH all three groups (p < 0.001)
Mean results of Serum Creatinine, Serum Urea & Serum Uric Acid were seen in the Euthyroid subjects, Subclinical & Overt hypothyroid patients.
Serum Creatinine: Mean levels were 0.77±0.11 mg/dL, 0.96±0.2 mg/dL, and 1±0.18 mg/dL. Significant differences were found between group I and groups II/III (p < 0.05).
Serum Urea: Mean levels were 21.5±6.2 mg/dL, 24.7±9.18 mg/dL, and 22.4±5.9 mg/dL. Significant differences were found between group I and groups II/III (p < 0.05).
Serum Uric Acid: Mean levels were 4.38±1.3 mg/dL, 6.5±1.61 mg/dL and 7.09±1.24 mg/dL. Significant differences were noted all three groups (p < 0.05).
Mean results of Urine Microalbumin, Urine Creatinine, Urine Albumin-to-Creatinine Ratio (UACR) & Estimated Glomerular Filtration Rate (eGFR) were seen in the Euthyroid subjects, Subclinical & Overt hypothyroid patients
Urine Microalbumin: Mean levels were 12.8±2.15 mg/L, 22.81±6.7 mg/L, and 34.84±12.5 mg/L.
Urine Creatinine: Mean levels were 112.3±9.85 mg/dL, 91±13.3 mg/dL, and 71.5±12.35 mg/dL.
Urine Albumin-to-Creatinine Ratio (UACR): Mean levels were 11.5±2.38 mg/g, 24±8.4 mg/g, and 44.5±16.96 mg/g.
Estimated Glomerular Filtration Rate (eGFR): Mean levels were 86±13, 66±20.4, and 61±15.9 mL/min/1.73 m².
There were statistically significant differences found in Euthyroid subjects, Subclinical & Overt hypothyroid patients (p < 0.001).
Correlations
Serum free T4: In the Overt Hypothyroid group, negative correlations were observed with UACR (r = -0.41, p < 0.05) and urinary microalbumin (r = -0.539, p < 0.001).(4)
Serum TSH: In the Overt Hypothyroid group, a weak positive correlation with urinary creatinine (r = 0.32, p < 0.05) was found. In the Subclinical group, TSH was positively correlated with serum uric acid (r = 0.32, p < 0.05) and urinary microalbumin (r = 0.43, p < 0.001).(Table 5)
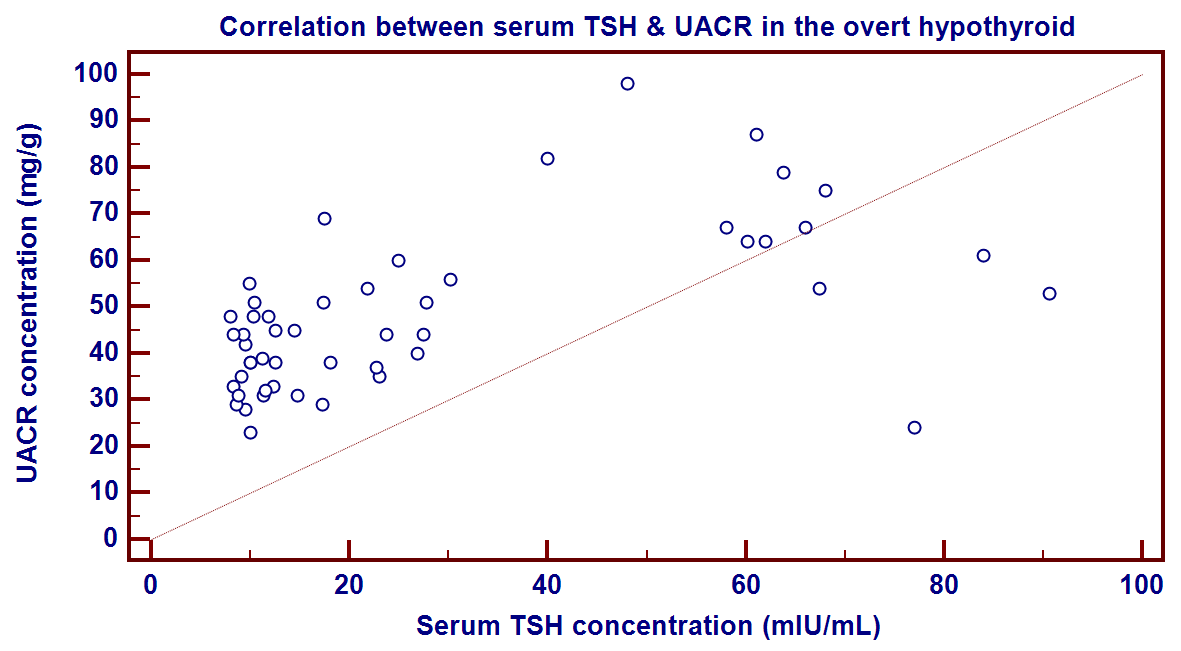
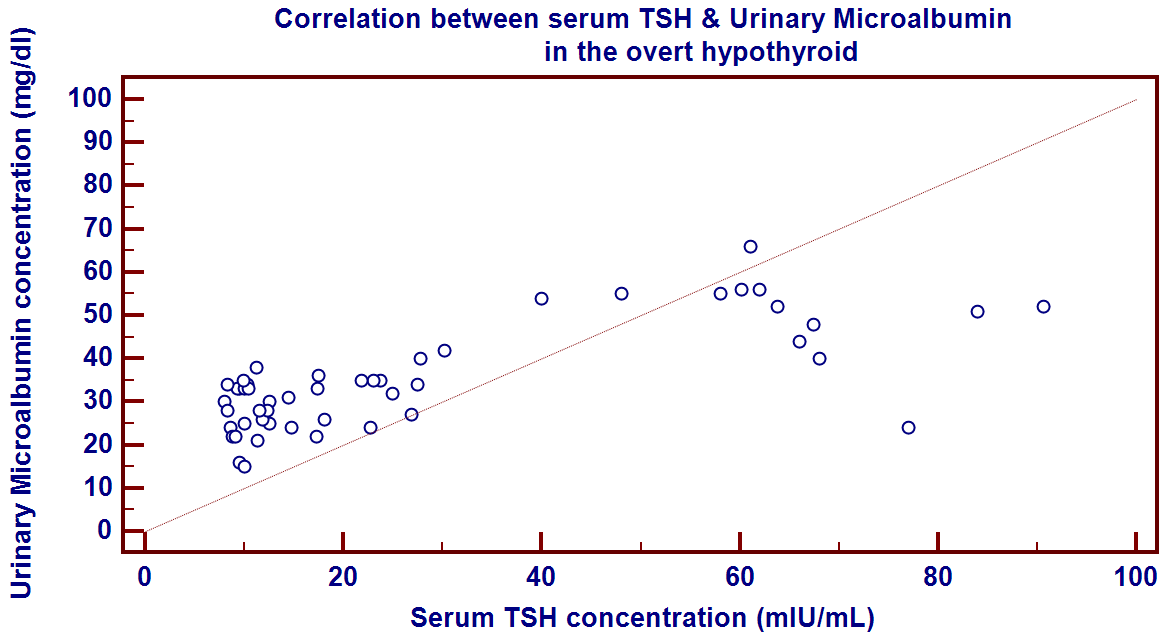
Table 4
Correlation of various parameters in different states of free T4
Table 5
Correlation of various parameters in different states of serum TSH
Discussion
The present study was done to evaluate the association between thyroid function and renal parameters among euthyroid, subclinical hypothyroid and overt hypothyroid individuals.
Thyroid disorders affect 200 million people worldwide. 1 According to various studies it has been estimated that around 42 million people in India suffer from thyroid disorders like Goiter, Hypothyroidism, Hyperthyroidism, Hashimoto’s disease and carcinoma of the thyroid gland. 2
In this study subjects were divided into three groups based on thyroid-stimulating hormone (TSH) and free Thyroxine (fT4) levels. Our findings show significant differences in biochemical parameters among euthyroid subjects, sub-clinical & overt hypothyroid groups, indicating potential renal impairment associated with thyroid dysfunction.
In sub-clinical hypothyroid group, 14 males and 46 females, in overt hypothyroid groups 13 male and 37 females, in euthyroid subjects 27 males and 83 females. The percentage rates of females are more than that of males.
The result of this study was similar to Ambika G U et al.,2 2011 who recorded that hypothyroidism was more frequent in females.
ANOVA comparison analysis
In our study, we found that the mean levels of serum urea and serum uric acid were statistically significant (p < 0.05). Additionally, serum creatinine, urine creatinine, urine microalbumin, UACR (urine albumin-to-creatinine ratio) and eGFR (estimated glomerular filtration rate) showed more statistical significance (p < 0.01). These findings were observed across the three thyroid groups: subclinical hypothyroid, overt hypothyroid, and euthyroid subjects.
Vaneet kaur et al., (2015),6 the study showed that there is a statistically significant rise in the levels of urea and creatinine in patients with subclinical and overt hypothyroidism as compared to euthyroid subjects.
The result of this study was likeTayal et al.,10 2009 who found that mean serum creatinine concentrations were significantly increased in both patient groups i.e. sub-clinical and overt hypothyroid as compared to euthyroid subjects. The levels of serum creatinine in hypothyroid subjects were within normal range (< 1.4 mg/dl) but significantly higher than in the euthyroid subjects (p<0.001).
The result of this study was agreed too with Aminul et al.,(2013),11 who found that serum creatinine level significantly higher in hypothyroid patients compared to controls.
Saini Vet al., (2012),12 Hyperuricemia has been observed in hypothyroid patients in other studies also. In hypothyroidism, hyperuricemia secondary to decreased renal plasma flow and impaired glomerular filtration.
Excretion function and hemodynamic of kidneys are changed, intrarenal vessels are contracted, the resistance of peripheral vessel is increased and the total volume of blood is decreased; this results in a reduction in renal blood flow, changing secretion function, tubular resorption, and a reduction in eGFR which is reversible by thyroxine treatment.
Pearson’s correlation analysis revealed several significant associations between thyroid hormones and renal parameters:
Free T3: In overt hypothyroid subjects, free T3 showed a significantly weak positive correlation with serum uric acid (p=0.03, r=0.3) and weak negative correlations with UACR and urinary microalbumin (p=0.04, r= - 0.27 &p= 0.02, r= -0.31). These findings suggest that lower free T3 levels may be associated with renal impairment and increased uric acid levels.
Free T4: In overt hypothyroid subjects, free T4 levels showed significantly moderate strong negative correlations (p=0.002, r= -0.412 & p<0.001, -0.539) with UACR and urinary microalbumin. This indicates that reduced free T4 levels are linked to increased markers of renal damage.
Serum TSH: In overt hypothyroid group, TSH levels showed weak positive correlations (p=0.04, r=0.28) with urinary creatinine, moderately strong positive correlations with UACR and urinary microalbumin (p=<0.001, r=0.57 & p=<0.001, r=0.72).
Serum TSH: In subclinical hypothyroid groups, TSH levels showed positive correlations with serum uric acid urinary creatinine, UACR, and urinary microalbumin (p=0.01, r= 0.32, p=0.00, r= 0.46, & p=<0.001, 0.43).
Sowmya et al., (2017), 13 a negative correlation between the FT3 and FT4 levels with microalbuminuria exists. Also, a significant association of subclinical and overt hypothyroidism with microalbuminuria is present. Overt Hypothyroidism was a strong and significant predictor of microalbuminuria compared to subclinical hypothyroidism in both univariate and multivariate analysis.
Tuliani TA. et al., (2017), 14 recent studies have shown that hypothyroidism is also independently associated with Microalbuminuria.
These correlations were strongest in overt hypothyroid subjects, suggesting that presence of microalbuminuria in urine is an early marker of renal impairment and micro vascular damage.
Vaneet kaur et al.,(2015),6 in patients with overt hypothyroidism, fT4 and fT3 did not show any significant correlation with any of these renal function parameters (serum creatinine, serum urea & serum uric acid). A statistically significant rise in uric acid levels has been observed in patients with overt hypothyroidism as compared to controls. But the rise did not correlate with any of the thyroid function tests.
In contrary, I have found significant weak positive correlation between the serum uric acid and TSH levels in subclinical hypothyroid groups.
Vaneet kaur et al., (2015), 6 TSH did not show any statistically significant correlation with any of the renal function parameters (serum creatinine, serum urea & serum uric acid) in subclinical hypothyroidism.
In this study, no significant correlation was found between the different thyroid groups and serum creatinine levels. This lack of correlation may be attributed to patients receiving treatment for hypothyroidism.
Pragaspathy V. et al., (2024), 15 a simple and practical MDRD and CKD-EPI equation for eGFR derived from serum creatinine, both of which showed a declining GFR compared with the control group, a p-value of <0.01. The altered eGFR levels in SCH suggest that kidney function may be of concern in patients with subclinical thyroid dysfunction.
In our study we found that eGFR values are significantly lower in sub-clinical and overt hypothyroid group as compared to euthyroid group, indicating decreased renal function p value (<0.05).
In our study, we found significant differences in mean results of serum creatinine, serum urea, serum uric acid, urinary creatinine, urine microalbumin and urinary albumin-to-creatinine ratio (UACR) in hypothyroid (Subclinical & Overt) patients as compared to euthyroid subjects. Estimated glomerular filtration rate (eGFR) values were significantly lower in both the subclinical and overt hypothyroid patients.
Hypothyroid groups compared to the euthyroid group. There was a strong and significant association between both subclinical and overt hypothyroidism and elevated levels of UACR and microalbuminuria. The presence of microalbuminuria in hypothyroid patients indicates widespread endothelial damage, which may be a consequence of the hypothyroidism.
Present study shows that there are increased levels of serum creatinine, uric acid, urine albumin creatinine ratio, urinary microalbumin levels and decreased eGFR levels in hypothyroid group as compared to euthyroid group. The prevalence of microalbuminuria and urine albumin creatinine ratio is high in overt hypothyroidism.
These changes in the biochemical values are because of the renal dysfunction evident by decrease in mean eGFR level as compared to mean eGFR level in euthyroid group. Hence, these findings clarify the interaction between thyroid gland and kidney showing the detrimental effect of hypothyroid state on renal functioning.
This renal impairment is often overlooked but is readily reversible by prompt treatment leading to normalization of biochemical markers Hence it is suggested that:
To assess the kidney functions of the patient at the time of diagnosis of Hypothyroidism.
To have strict observation of these parameters in cases especially in person having risk factors of developing kidney diseases or impairment. e.g.-hypertension, diabetes mellitus.
To do Thyroid function test in patients having these biochemical abnormalities and patients having worsening chronic renal failure without any causes.Ethical approval has taken for research.