Introduction
Neonatal Septicemia (NS) is deadly illness, and perceived reason for morbidity and mortality in the neonates (i.e., youngster under 28 days1) around the world. Neonatal Septicemia is the third driving reason for neon atal mortality and is accountable for 13% of all neonatal mortality & 42% of Neonatal deaths in the first week of life.2 NS essential side effects are non- specific and associate with the non-infective causes which make it challenging for timely detection. The symptoms of Neonatal Sepsis can be clinically indistinct from different noninfectious conditions like respiratory distress syndrome or maladaptation. Hence it is very crucial to detect timely and prevent the adverse outcomes.
Blood culture (BC), Hematological S coring System (HSS) and C-reactive protein (CRP) are three well identified parameters indicated for analysis of Neonatal Sepsis3 or infection.
Blood Culture is considered as the Gold Standard in detecting Neonatal Infections. But still the consequences of Blood Culture get affected by blood sample getting vaccinated, usage of pre-natal antibiotic, level of bacteremia and laboratory facilities. Hence its rate of positivity is relatively low. Also in the case of Sample volume, the mentioned minimal blood volume for blood culture in newborns is only 1ml. However in most cases the sample volume collected is found to be only 0.5ml. In low-colony count bacteremia, around 60% of blood cultures will be falsely negative with 0.5 ml sample volumes. Multiple blood culture could benefit the augmentation of this test, but past studies conducted in the neonatal period have shown that diagnostic tests like blood culture are time consuming as well as show conflicting results.2
Hematological Scoring System (HSS) can improvise the diagnostic accuracy of the complete blood cell count as the absolute screening test for Neonatal sepsis. But it is highly challenging to interpret the neonatal period because it varies considerably with the day of life and the gestational age.
Low values of white blood cells, low values of absolute neutrophil counts and high immature or total ratio are related to early onset of sepsis in infants. High or low white blood cell counts, high absolute neutrophil counts, high immature /total ratio and low platelet counts are related to late onset of sepsis. Though all of these mentioned parameters are linked with sepsis or infection, all of these conclusions have low sensitivities.
Past few decades a variety of Sepsis Markers have been introduced for the laboratories to evaluate and improve the detection of sepsis but unfortunately none of them could give a confirm 100% diagnosis.
C-reactive protein (CRP) is one of the accurate laboratory sepsis marker contemplated until now. In spite of the fact that there is continuous up and down of new infection markers CRP still remains the ideal index in laboratory detection of sepsis. CRP was detected by Tillet and Francis in 1930 from the sera of patients diagnosed with acute infection with a non-protein pneumococcus extracts called C- polysaccharide in the presence of Calcium ions. Philipson and Hanson (1981)4 have further emphasized the role of CRP in bacterial infection in Neonates.5
CRP is a member of the Pentraxin family of Proteins which are synthesized in the hepatocytes. The structure of CRP, including Calcium phosphorylcholine binding sites facilitate the CRP to identify and bind to a variety of biological substrates. These substrates include phosphocholine and phospholipid components of the damaged walls of the cell, chromatin matter and the nuclear antigens resulting in the formation of CRP ligand complexes. Here CRP binds directly to the neutrophils, macrophages and other phagocytes, stimulating an inflammatory response and the release of cytokines.5
Since CRP level shows a detectable increase after 3 days of birth and low level in premature infants, using a single value for all infants with infection may be suboptimal. CRP is the most sensitive of all the acute phase proteins with levels rising as much as 1000 fold during an acute inflammatory condition. As sepsis is the most treatable cause of inflammation in the neonates, an increased CRP has been a useful marker for sepsis in many studies. CRP is a good indicator in detecting the Neonatal infection and guiding the line of treatment for along with other diagnostics tests in the management of the sepsis patient. Numerous authors have preferred C-reactive protein as a highly sensitive, indirect indicator of sepsis in neonates.6
The present study was conducted to review the role of CRP as a diagnostic parameter along with HSS in neonatal infections. The purpose was to obtain range of tests that are fast, efficient, feasible and practically possible for laboratories with small setups in the developing as well as developed countries.
Materials and Methods
The study was conducted at Dr Godbole laboratories, Pune during the month of March to April 2019 in collaboration with scientific team of Transasia Biomedicals Limited, Mumbai. Sixty patient samples were included in the study among which 20 samples were from normal individuals that were considered as control samples. The age range of neonates was from 1 day to 21 days. All the patients have given serum as well as EDTA whole blood sample for testing. The samples were collected as per national and international sample collection guidelines.
The EDTA whole blood sample was used for complete blood count (CBC) examination. HSS mentioned by Rodwell (1988)4 were us ed in this study which comprises of white blood cell and platelet count, white blood differential count, nucleated red blood cell count, assessment of neutrophil morphology for degenerative changes.7 Serum samples were used for analysis of CRP. Blood samples of 2 ml were obtained from peripheral veni-puncture in all the neonates with infection within 24hours of admission before administration of antibiotic therapy. These blood samples were then transferred into a plain tube to obtain serum and in EDTA tubes to obtain whole blood.
A multicenter study was conducted by WHO in 2008 on Neonatal infection in which the algorithm of seven signs and symptoms for Neonatal Sepsis was emphasized. In our study we have considered all these seven symptoms while enrolling patients for the study.8
The CRP test was performed on EM-200, a fully automated biochemistry analyzer and reagents from Erba Mannheim & Transasia Biomedicals Limited, Mumbai. The reagents were based on quantitative detection of C- reactive protein (CRP), in human serum or plasma by Latex-enhanced turbidimetric immunoassay. The quality controls were assayed before analysis of patient samples. All the quality controls are found in the range. The analysis for statistics was done on MS office platform using CRP, HSS and blood culture as parameters for analysis. The Spearman’s correlation was used and p-value of <0.05 were considered as statistically significant.
Table 1
Results
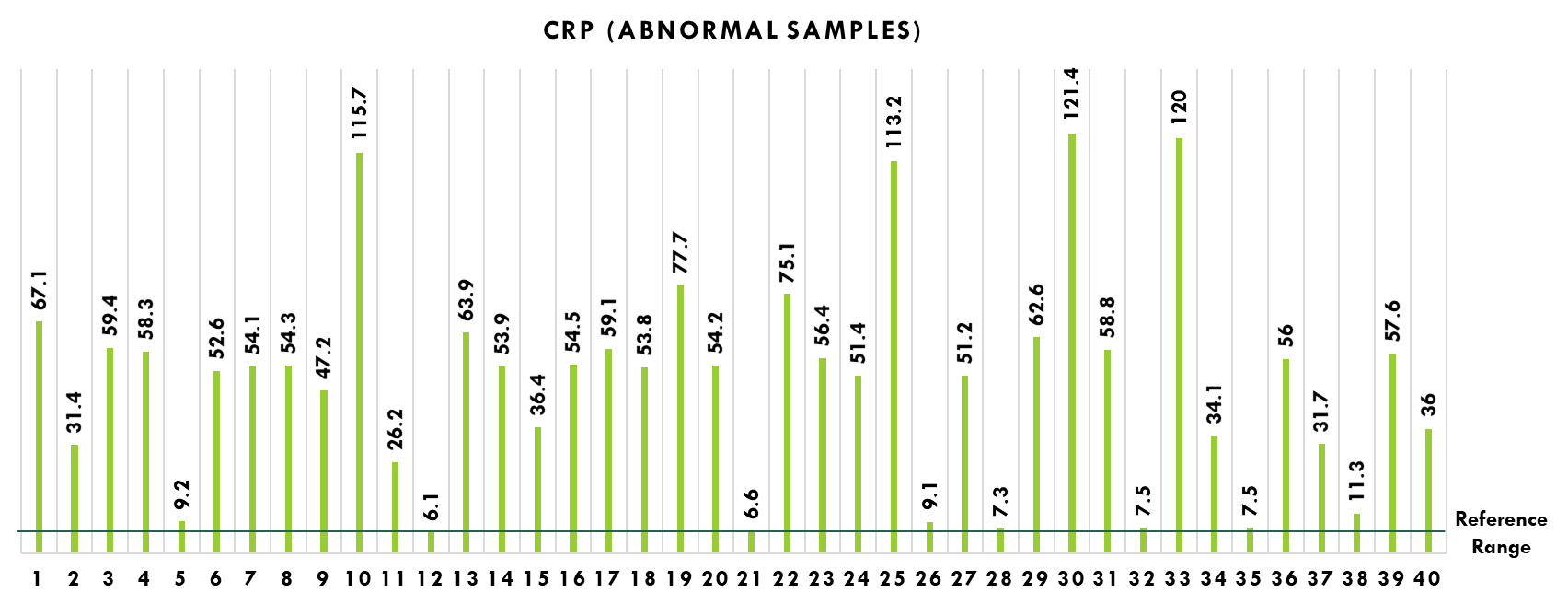
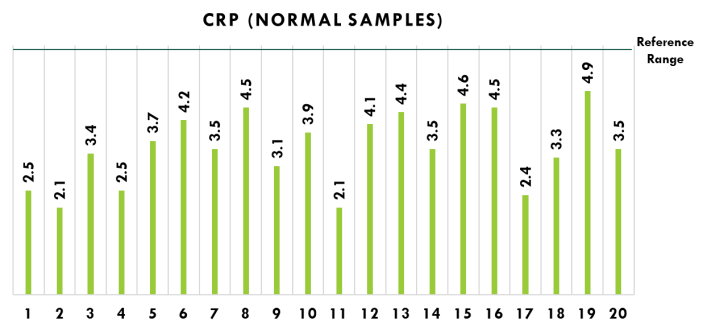
All the neonates were less than 28 days old. The average age for normal patients was 10 days ± 6 days and for abnormal patients was 7 days ± 4 days (p = 0.015). The reference range for CRP was 6 mg/L as per the kit insert given by manufacturer. All the 40 abnormal samples were found above the given reference range and all the normal samples are below reference range. (Figure 1,Figure 2)
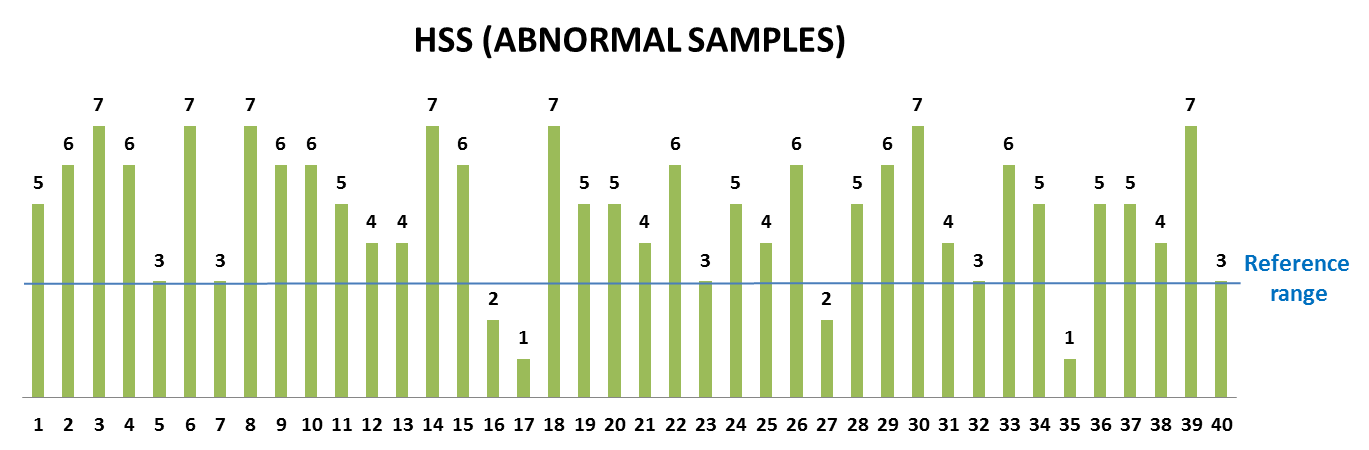
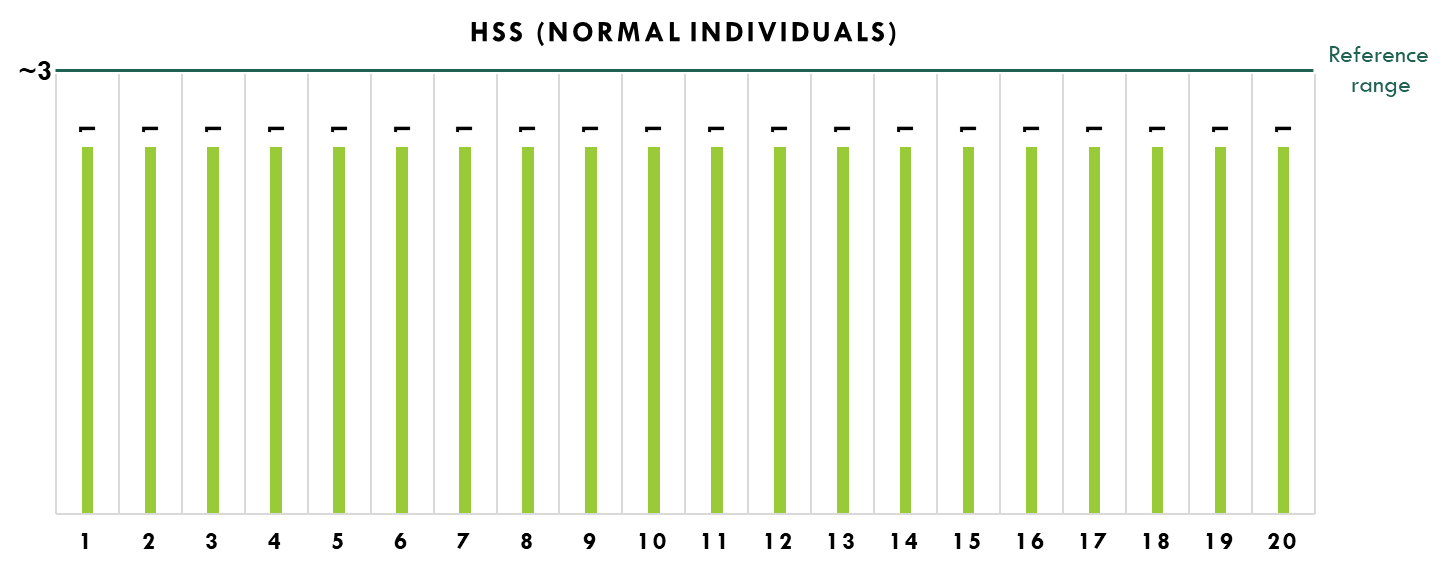
The HSS should be greater than 3 to be considered as sepsis infection.9 Among the abnormal sample 4 individuals were found to be in below the reference range and in normal samples all the individuals were below the reference range. (Figure 3,Figure 4)
Discussion
Neonatal Infection is a lethal clinical condition in which early diagnosis is very difficult. Various inflammatory markers were used to diagnose Neonatal Infections so as to reduce the mortality and morbidity in neonates. The blood culture test is considered to be the gold standard but in most cases its non-availability in most peripheral setups, higher cost more chances of contamination and delayed results was observed. In 2011, Narsimha et al has published data on significance of HSS in early diagnosis of neonatal infection in which HSS is considered as a simple, quick, cost effective tool for early diagnosis of neonatal sepsis.
In current observations, HSS has given false negative results in 4 abnormal cases (10%), and 100% results were showing abnormal results in CRP values. In spite of all this, still it is recommended to rely on both clinical correlations and laboratory findings to confirm the diagnosis. CRP can be done in all those neonates who are on prior anti-microbial therapy. In our study 40 neonates were proved to have neonatal sepsis which was based on signs and symptoms shown by patient. The other studies have revealed, CRP biochemistry assay have high sensitivity and specificity as compare to HSS for diagnosis of NS; we also got 100% sensitivity and specificity for CRP testing. Our results are comparable with the study done by Anwar Zeb Jan, et.al in which CRP was positive with the sensitivity, specificity, negative and positive predictive values of 94.01%, 69.17%, 79.29%, 90.19% respectively. Hence, we conclude that CRP is a good diagnostic marker for the infection in neonates at the time of initial assessment. Similarly, the study done by William E, Benitz et al shows CRP had higher sensitivity 92.9% and 85% for proven and probable sepsis and 78.9% and 84.4% for proven sepsis in early and late onset episodes.10 In our study we used quantitative assay for CRP estimation which is less time consuming and effective in analyzing samples of neonates who are already on antibiotics treatment.
However, Nora Hofer, et al, has recommended CRP as a safer compared to other, newer markers for NS. In same study need of further research on the topics of the influence of gestational age on CRP kinetics in infection, non-infection confounder, and evaluation of dynamic and gestational age dependent reference values was necessitated. Although in our study, results are showing high sensitivity and specificity CRP, we also recommend further analysis of more number of samples along with other diagnostics markers such as PCT, IL6, IL8, CD11b, and CD64, etc. to improve diagnostics accuracy in neonatal infections.
Conclusion
CRP is one of the reliable diagnostic markers used in diagnosis of neonatal infections that has been widely available, most studied and preferred over the newly emerging infection markers. Even CRP assay has proven to be less time consuming and effective for analyzing samples of neonates who are already on antibiotics treatment. Further studies are recommended for clinical correlation of CRP values and other laboratory findings with higher number of samples for the diagnosis of neonatal infections.6